Beyond the Primary User: The Rise of the B2B2C “Caregiver Tech” Stack
Introduction
In the United States, population aging is reshaping how caregiving responsibilities are distributed. According to estimates from the National Alliance for Caregiving and AARP, more than 50 million American adults reportedly serve as informal caregivers for an older relative or a person living with a disability [Source A]. The healthcare system—fragmented across Medicare (federal insurance for adults 65+), Medicaid (coverage for low-income individuals), and a wide array of private providers—relies heavily on this unpaid labor (established fact).
A category of technology solutions is emerging in response, focusing not on the older adult as an isolated user but on the senior–caregiver dyad. These tools—referred to here as the Caregiver Tech Stack, a set of functional layers dedicated to care coordination—are most often delivered through a B2B2C model (Business-to-Business-to-Consumer: a vendor sells to an intermediary organization that then provides the tool to the caregiver). This article examines the forces shaping this shift, the functions covered by the stack, why B2B2C is gaining traction in the U.S., and the constraints that frame its development.
1. Shifting the “Primary User”: From the Isolated Senior to the Senior–Caregiver Unit (U.S. context)
For a long time, aging-related technologies targeted the older adult as the primary user: medical alert systems, tracking apps, telehealth platforms. This paradigm assumes a user who is autonomous and digitally capable. Yet a substantial share of people aged 75+ experience cognitive or functional limitations that reduce this capacity (source needed).
The conceptual shift is to recognize that the functional unit of care is the senior–caregiver dyad, often extended to a network including geographically distant relatives, home care aides, and clinicians. The primary user of the technology is therefore often the caregiver (hypothesis). Interfaces, information flows, and consent models must reflect this reality.
2. Caregiver Burden as a Systemic Problem (definition + mechanisms)
Caregiver burden refers to the physical, emotional, financial, and social strain associated with ongoing informal caregiving, and it is linked to higher rates of depression and morbidity among caregivers (established fact). According to the AARP Public Policy Institute, the annual economic value of unpaid informal care in the U.S. is estimated in the hundreds of billions of dollars [Source B].
Three mechanisms amplify this burden in the American context. First, care pathways are fragmented: caregivers must navigate multiple providers, distinct insurance regimes, and poorly coordinated community services (source needed). Second, there is no universal formal care coordination: no coordinator is systematically assigned to older adults with dependency-related needs (established fact). Third, informational isolation persists: caregivers often lack awareness of available resources, including LTSS (Long-Term Services and Supports) and HCBS (Home and Community-Based Services, partially funded through Medicaid) (source needed).
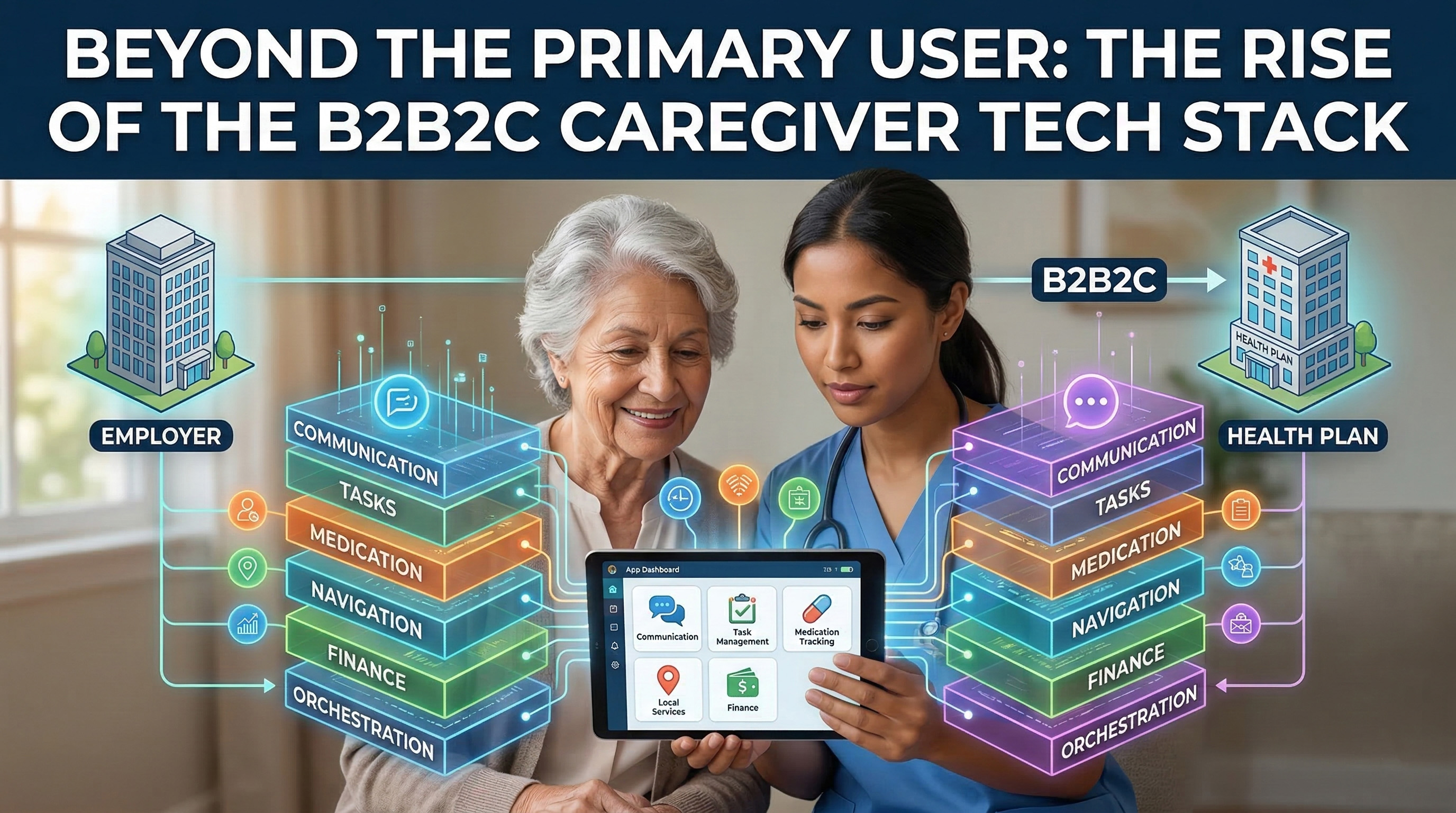
3. Mapping the “Caregiver Tech Stack” (functional layers)
The notion of a “stack” refers to an articulated set of functional layers. Six layers can be distinguished.
3.1 Communication and coordination
Secure messaging, shared activity logs, and notifications across the care network. The goal is to replace untraceable verbal handoffs with documented exchanges (established fact).
3.2 Task and routine management
Daily planning, reminders, and check-ins. A care plan can be formalized, distributed across contributors, and updated collaboratively (established fact).
3.3 Medication and appointments
Medication reminders, adherence tracking, and appointment scheduling. This layer becomes critical during transitions of care—moves between hospital, home, and rehabilitation—when the risk of error is high (established fact).
3.4 Navigation of local services
Aggregation of accessible resources: Medicaid eligibility, HCBS programs, transportation, meal delivery, mental health support. Navigation centralizes information otherwise scattered across agencies (established fact).
3.5 Financial and administrative oversight
Expense tracking, bill management, and insurance coordination. Access to the financial data of a vulnerable person requires an appropriate legal framework—power of attorney or guardianship—defined at the state level (established fact).
3.6 Orchestration and access governance
Under HIPAA (Health Insurance Portability and Accountability Act), health data sharing depends on parties’ status: obligations apply to covered entities and their business associates, while caregiver access is conditioned by personal representative status or a patient-specific authorization (source needed). Platforms must define differentiated access roles. Interoperability with electronic health records remains a major technical challenge (established fact).
Vignette A — Without a stack. A long-distance caregiver coordinates her 82-year-old mother’s daily life by phone. She learns after the fact that a cardiology appointment was missed. During a hospitalization, no medication information reaches the clinical team. Discharge happens without a transition plan.
Vignette B — With a stack. A shared journal, automated alerts, and an authorized-access care plan reduce information breakdowns. The medication list is viewable within consented permission boundaries. The transition back home is formalized and visible to the network.
4. Why B2B2C Is Becoming Dominant in the United States (employers, home care agencies, health plans)
Direct-to-caregiver sales (B2C) face obstacles: high acquisition costs, weak retention, and caregivers’ already-saturated cognitive load (hypothesis). Out-of-pocket payment is an added barrier for caregivers under financial strain (established fact).
B2B2C introduces a third-party payer-distributor. Three buyer categories are emerging. Employers incorporate caregiver benefits into their benefits packages; caregiver-driven absenteeism and productivity loss reportedly create substantial annual costs [Source C]. Health plans, including Medicare Advantage plans and Medicaid managed care programs, seek to reduce avoidable hospitalizations (established fact). Home care agencies may use these tools to strengthen family coordination (hypothesis).
5. Product and partnership implications (U.S. healthcare + benefits) — without naming brands
Motivation asymmetries generate concrete friction points. Employers aim to reduce absenteeism; insurers demand evidence of clinical impact; caregivers seek relief but resist intrusive prompts; older adults may refuse certain sharing levels to preserve autonomy. These tensions tend to crystallize around access permissions, check-in cadence, clinical escalation protocols, and the scope of shared data (established fact for divergence of interests; hypothesis for stack-specific mechanisms).
The distinction between care coordination—logistics, information, planning—and caregiving—hands-on support—is decisive. Technology optimizes information flow (established fact). It may help limit certain errors during transitions of care (hypothesis). However, it does not replace physical assistance, continuous presence, or the relational work involved in day-to-day support (established fact).
6. Limits and controversies (risk, adoption, equity, privacy, liability)
Disguised surveillance. Tracking features can function as surveillance of the older adult. When cognition declines, capacity to consent diminishes. Consent should be treated as a continuous, revisable process, including periodic reassessments and, when needed, involvement of a legal representative (established fact). The lack of a unified federal framework for digital consent in cognitive decline represents a gap (hypothesis).
Equity of access. B2B2C may reproduce inequality: caregivers at employers offering generous benefits gain access, while precarious caregivers do not. Caregivers from ethnocultural minority groups—who often carry heavier caregiving loads—have less access to employer programs (source needed). Access via Medicaid remains to be built (hypothesis).
Digital divide. Adoption presumes device access and minimum digital literacy—conditions not universally met, especially in rural contexts (source needed).
Legal liability. In the event of failure (missed alert, facilitated error), responsibility allocation among caregiver, vendor, and distributor remains legally indeterminate (hypothesis).
Insufficient evidence. Effectiveness data remain limited. Three methodological requirements stand out: (a) measure precise outcomes (readmissions, medication adherence, caregiver stress), (b) use robust designs (pragmatic trials, quasi-experimental comparisons), and (c) evaluate over time horizons that capture effects on dependency trajectories. Much of the available evidence derives from internal data not independently evaluated (hypothesis).
Conclusion
The rise of a caregiver-centered tech architecture delivered through B2B2C reflects a growing recognition: informal caregivers are central actors in the U.S. healthcare system, not invisible auxiliaries (established fact). By shifting the primary user toward the senior–caregiver dyad, these tools acknowledge a functional reality that public policy still struggles to formalize.
Technology can optimize coordination, but it does not resolve the home care workforce shortage, LTSS underfunding, or the intrinsic exhaustion tied to hands-on caregiving. B2B2C may facilitate distribution, yet it also introduces tensions among institutional buyers, caregivers, and older adults. The challenge is dual: generate rigorous evidence of effectiveness and ensure these tools support older adults’ autonomy as much as they support the performance goals of the organizations that fund them.